


What are Meniscal Injuries? Here is an article on meniscal injuries. Enjoy, and let me know what you think.
The knee joint, classified as a hinge joint, is one of the largest and most complex joints supporting the human body.
The importance of this specific joint to everyday activities is indisputable. For any adult with a healthy knee joint, walking, running, and squatting is tasks that require little effort. Since the knee is used frequently, it is vulnerable to injuries, overuse, and degeneration.
Meniscal injuries are the leading cause of disability directly related to the knee.
A meniscal injury refers to tearing any of the two menisci of the knee. A meniscus is commonly described as a rubbery, crescent-shaped piece of cartilage that functions as the main shock absorber in the knee joint. This structure cushions the two prominent bones making up the knee joint: the thigh bone and the shin bone.
When someone says they are suffering from a torn knee cartilage, they refer to a meniscal injury.
Meniscal tears can occur in many ways. The most common active ones result from solid or forceful twisting motions. There are other ways that a meniscus injury can occur, and I will go through those in a later article. A meniscal tear is classified based on its gross appearance and location and the meniscus. The different descriptions are thoroughly discussed in the succeeding articles. 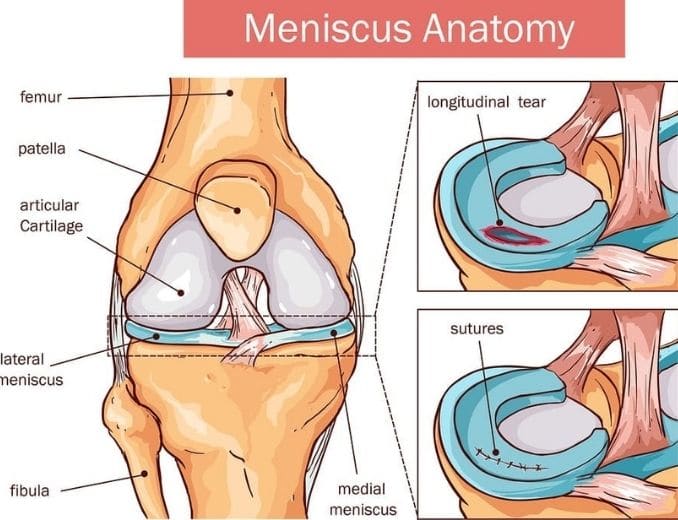

A meniscal injury is a knee injury that occurs in many individuals. Meniscal damage commonly occurs with knee injuries, such as tearing the anterior cruciate ligament. Although athletes engaged in contact sports are more widely recognized as at risk for meniscal injury, anyone can suffer from a meniscus tear at any age.
Meniscal injuries may significantly disrupt daily activities.
The meniscus weakens with age as well. For this reason, older adults may suffer from a meniscus injury even when they initially only had a minor knee injury. These signs and symptoms may not be life-threatening. Still, without the right interventions, meniscal injuries may significantly disrupt daily activities, reduce function, cause pain, and lead to reduced quality of life.
The understanding and appreciation of the menisci concerning the biomechanics of the knee have drastically changed since Sutton described these structures as of no use in the 1960s. Given the limited understanding of its importance to knee biomechanics, doctors commonly completely removed the meniscus once its integrity was in doubt.
Today, people regard the menisci as the vital structure of the knee. Along with this development, the diagnosis, treatment, and rehabilitation of meniscal injuries have radically changed.

These articles introduce the basic concepts of a meniscal injury, focusing on its treatment and rehabilitation through exercise.
More and more research and client feedback support the importance of an effective exercise program in recovering from a meniscus injury to regain function, decrease pain, overcome knee catching, improve knee movement and increase knee strength. Besides strengthening and stretching, a meniscus injury workout requires much more. In the following articles, we will go into the components.
Anatomy of the Knee and the Menisci
The meniscus cushions the thigh and shin bone. Before thoroughly discussing this vital structure of the knee, it is essential to understand the anatomy of the knee joint. What systems makeup one of the largest joints in the human body? How do these structures support the movements involving the lower extremities?
Overview of the Knee Joint
We recognize the knee joint as the largest joint in the body. The knee joint is classified as a hinge joint like the elbow joint. A joint is where two or more bones meet to allow movement. A hinge joint is a type of joint where a bulging outer part of one bone fits into an inward curved-like surface of another bone. This specific type of joint only allows motion in one plane or a backward and forward movement.
Let’s look at an overview of the knee joint. The knee joint consists of four bones and a broad network of ligaments, structures connecting bones to other bones and muscles.
Bones of the Knee Joint
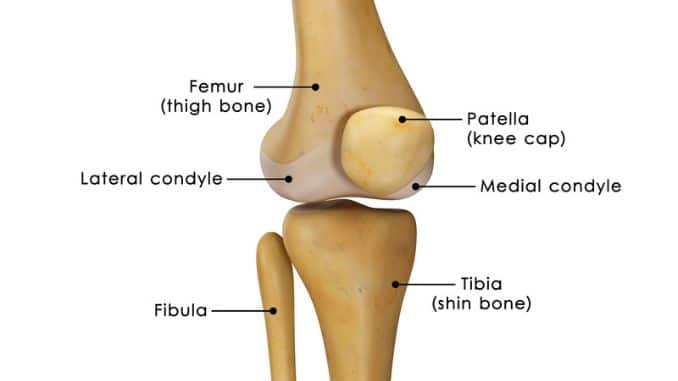
The knee may appear like a non-complex joint, but it mainly consists of four bones:
- femur
- tibia
- fibula
- patella
The femur, or the thigh bone, is the most prominent bone in the lower extremity. Ligaments attach it, and a capsule to the tibia is commonly called the shin bone. Running parallel to the tibia is the fibula.
The major movements of the knee joint occur between the femur, the tibia, and the patella. A protective structure called the articular cartilage covers these bones. The cartilage decreases the frictional forces every time the bones of the knee move.
Ligaments of the Knee
The stability of the knee is primarily attributed to the ligaments.
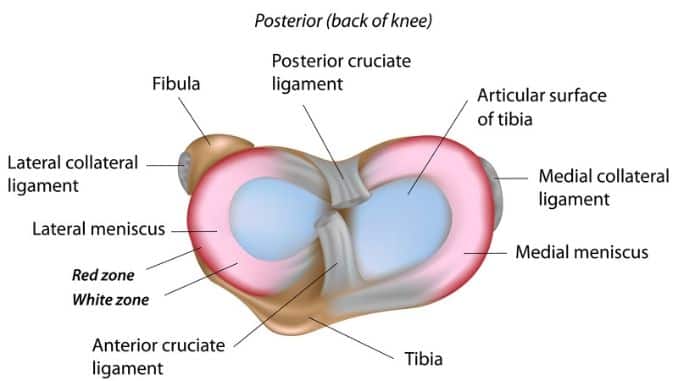
There are four main ligaments found in the knee joint:
- anterior cruciate
- posterior cruciate
- medial collateral
- lateral collateral
The anterior cruciate ligament, or ACL, must be discussed further among these ligaments. Meniscal tears commonly occur associated with an ACL disruption, specifically on the lateral side of the knee (New England Musculoskeletal Institute, 2011). Injuries involving the menisci occur with ACL tears up to 70% of the time (Wright State Physicians, 2012). The ACL forms right in the middle of the knee. It runs from the front of the shin bone to the back of the femur. The ACL functions to inhibit the tibia from making the excess forward motion. Twisting motions are the most common cause of ACL injuries.
Articular Cartilage
The articular cartilage is a smooth tissue that encloses the ends of bones making up the knee joint. In the knee, the articular cartilage facilitates the gliding of the bones of the knee without causing damage or excessive friction to the surfaces.
The menisci protect the articular cartilage of the knee from sustaining excessive pressure on one surface area on the joint’s surface. In the absence of the menisci, the forces applied to the knee are not effectively transmitted. The pressure is applied more intensely to one region, eventually leading to the wearing and tearing of the articular cartilage, as seen in osteoarthritis.
Knee Joint Capsule
The knee joint capsule is described as a thick and rigid structure that surrounds the entire knee joint.
A synovial membrane that lines the inside of the capsule produces the synovial fluid, which functions as a lubricant. The surrounding ligaments further reinforce the knee joint capsule.
Menisci
Each knee joint comprises two menisci, the wedge- or crescent-shaped structures found between the two major knee bones: the thigh and shin. In the cross-section, the menisci are triangular. The upper surfaces of the menisci are in contact with the round prominences of the thigh bone; the lower surfaces of the menisci make contact with the plateaus of the shin bone.
The C-shaped medial meniscus lies on the inner edge of the superior surface of the tibial bone.
The lateral meniscus found on the outer edge of the knee is almost circular. The lateral meniscus covers a broader portion of the tibial plateau surface than the medial meniscus.
Reports showed that the medial meniscus does not demonstrate a direct connection to any muscles in the lower extremity (Bhagia, 2012).
Function of Menisci
These fibrocartilages function as effective shock absorbers of the knee. The menisci’s back or the posterior parts absorb most of the pressure every time the knee bends (Orthogate, 2011). The menisci efficiently spread out the forces transmitted across the knee joint, making them crucial structures in maintaining the correct weight distribution between the tibia and femur.
Mobility of the Menisci
The medial and lateral menisci anchor to the other supporting structures of the knee. Despite the attachments, the menisci are mobile. The degrees of their mobility are not the same, however. Baker (2011) found that the medial meniscus is only half as mobile as the lateral meniscus. The looser attachment of the lateral meniscus to the capsule explains its greater mobility. Researchers think that the excursion or mobility of the lateral meniscus exceeds more than 10 millimeters.
The posterior horn of the medial meniscus has the most significant risk for disruption (Baker, 2011). The medial meniscus’s slight degree of mobility may be attributed to its injury vulnerability.
Water and Collagen Component
Water is the major component of the meniscus, comprising 70% of the total wet weight of the fibrocartilage (Athanasiou & Sanchez-Adams, 2009). At dry weight, collagen, specifically type 1 collagen, makes up 75% of the total weight of the meniscus. A collagen group of insoluble fiber proteins forms the structures supporting and connecting the tissues. Type 1 collagen fibers arranged in the circumferential direction endure the meniscus’s tensile strength during weight-bearing and shock absorption. It is approximated that there are nearly 30 types of collagen in the body.
Blood Supply
An adequate blood supply is essential to repair and heal any bodily tissue—the lesser the blood supply, the slower the healing time, or the poorer the prognosis. The circulating blood distributes the nutrients and elements required for healing; thus, it is essential to be familiar with the blood supply to the menisci to understand a meniscus injury’s potential response to treatment and rehabilitation.
The meniscal blood supply is limited to its outer edges or margins. The remaining areas lacking blood supply obtain the nutrients required for repair from the synovial fluid, a lubricating fluid found in the cavities of joints. Areas lacking blood supply rely on passive diffusion and mechanical pumping to receive nutrients.
Arnoczky suggested a classification system that categorizes meniscus lesions concerning the meniscal blood supply. As an overview, the red zone obtains a sufficient supply of blood, and the white area does not.
Red-red tear
The red-red tear occurs in the red zone, recognized as a blood-rich area. In this type of tear, both sides obtain an available blood supply, a condition that promotes good healing.
Red-white tear
The red-white tear includes the meniscus’s outer rim and middle part. In this type, one end of the tear receives adequate blood supply, and the other is in an area that lacks a sufficient pool of blood.
White-white tear
We find the white-white tear wholly in the middle part of the meniscus, where blood supply is lacking. As a consequence, repair and healing are not favorable.
Later this week, I will be releasing the Meniscus Tear Solution:
Rick Kaselj, MS
If the above article interested you, this article may as well:
- What to do About a Meniscus Tear?
- What Came First, the Meniscus Injury or Osteoarthritis?

